
Plenty. It’s our opportunity to make a quantum leap forward.
Legal Evolution readers are likely familiar with law firm competency models that define the skills and capacities of their lawyers, including the stages of development. In response to changes in the accreditation requirements, law schools have been slowly moving toward what is called Competency-Based Legal Education (CBLE). See, e.g., Michele R. Pistone, “Competency-based legal education,” Christiansen Institute, Mar. 29, 2016.
CBLE is an outcomes-based approach to the design, implementation, assessment, and evaluation of legal education programs, using an organizing framework of competencies. A competency describes a key set of abilities required for someone to do their job. As of mid-July of 2020, 186 of the 194 ABA-accredited law schools have published learning outcomes on their websites as a first step in the process of moving toward CBLE, all of which are available through a database maintained by the Holloran Center, a research center I co-direct at the University of St. Thomas School of Law in Minneapolis.
As we move into this new phase of legal education, we have an opportunity to take advantage of medical education’s “lessons learned,” as they’ve been on this journey for more than two decades. Arguably, one of the biggest insights is that the shift from time-based to competency-based education is massive in scope and complexity and thus remains an ongoing project. See Dr. Eric Holmboe & Dr. Robert Englander, “What Can the Legal Profession Learn from the Medical Profession About the Next Steps?,” 14 U. St. Thom. L. J. 345 (2018) (summarizing progress since the late 1990s). Thus, the one clear lesson for legal education is that movement toward competency-based education will also be a decades-long process.
To prepare us for this journey, this post dives into the details of the medical field’s experience with competency-based education, which started with an urgent need to deal with issues of inadequate quality of care. After reviewing the origins and maturation of the new medical education competency-based model, I explore how it might be applied to legal education.
Responding to a serious quality problem
In the 1980s and 90s, concerning signals of problems in the quality and safety of healthcare percolated through the healthcare system.
By the late 1990s, the medical education community realized that one of the root causes was the failure to sufficiently prepare students to meet the challenges of a dynamic and changing healthcare system. Medical educators came to understand that a principal emphasis on medical knowledge and cognitive skills was inadequate to meet patient and population needs. The earlier approach of “if you are really smart cognitively, you’ll be fine” was not sufficient. Holmboe & Englander, supra, at 347. Medical educators recognized the central importance of a much broader framework of patient-centered care where cognitive technical skills were necessary but not sufficient to meet patient and healthcare system needs. See Institute of Medicine, Crossing the Quality Chasm (2001).
The medical education enterprise had to start by identifying the needs of the patients and the healthcare system and then working backward to defining the critical competencies that each medical student would need to develop and demonstrate before becoming licensed. Drs. Holmboe and Englander note:
The next stage of evolution in the thinking of the medical education community, after defining the core competencies, was to develop a model of how the learner should proceed through a series of developmental stages in each competency. The resultant strategy was to adjust curriculum and assessment to facilitate that developmental progression.
Holmboe & Englander, supra, at 350. Fortunately, this Competency-Based Medical Education (CBME) is rapidly being adopted across the globe. See Elaine Van Melle et. al, “A Core Components Framework for Evaluating Implementation of Competency-Based Medical Education Programs,” 94 Acad. Med. 1002-09 (2019).
Based on competency rather than time
CBME is a different model from traditional education where the emphasis has been on student completion of a certain number of exposure hours of credit (called a tea-steeping model where the student is like a teabag in a cup of hot water for the right amount of time). See Brian David Hodges, “A Tea-Steeping or i-Doc Model for Medical Education?,” 85 Acad. Med. S34 (Sept. 2010).
Table 1 below summarizes the major differences.

Evaluating the design of CBME programs has been hampered by the lack of a clear shared understanding of what are the most important components of a CBME program.
In an effort to achieve relative consensus, 59 members on an international CBME expert panel recently engaged in a multi-stage process that combined scholarship from education theory and medical education. The result was the identification and organization of CBME into five core components, which is summarized below in Table 2.
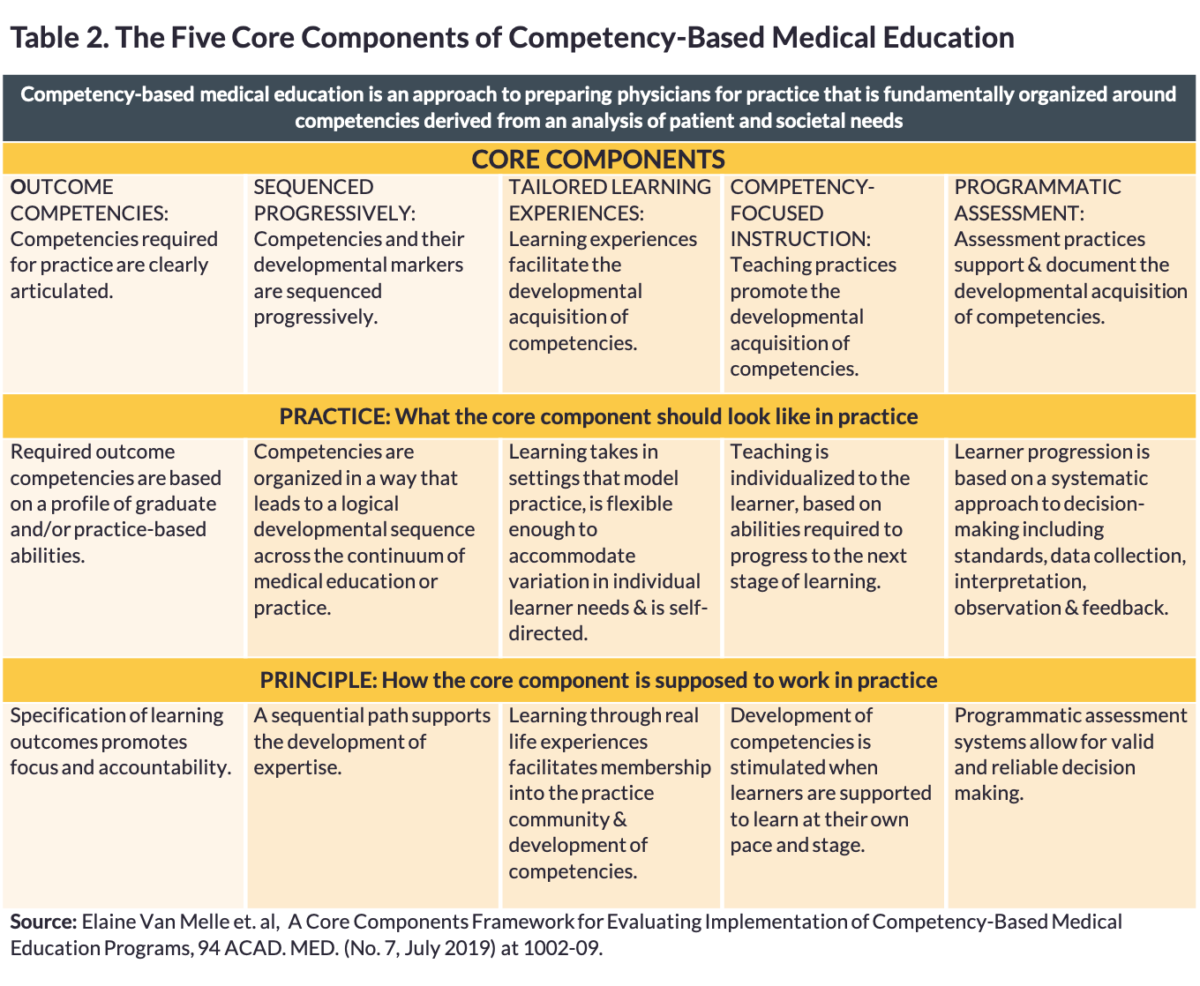
 Of the five core components in Table 2, the expert panel envisioned “Outcome Competencies” and “Sequenced Progressively” as the central core components guiding competency-based medical education. Figure 1 shows the centrality of these two components.
Of the five core components in Table 2, the expert panel envisioned “Outcome Competencies” and “Sequenced Progressively” as the central core components guiding competency-based medical education. Figure 1 shows the centrality of these two components.
Applying the CBME frameworks to law
A simple and worthy thought experiment is to consider how the CBME frameworks, with very slight modifications, could be applied to the education of lawyers.
If so, the first central core component of CBLE requires identifying the needs of clients and the legal system and then specifying core-competency learning outcomes that each student must develop and demonstrate to meet these needs. A major challenge facing law schools is the paucity of quality data on the core competencies needed by clients, legal employers, and the legal system. See Neil W. Hamilton, “The Gap Between the Foundational Competencies Clients and Legal Employers Need and the Learning Outcomes Law Schools are Adopting,” 89 UMKC Law Rev. __ (2020). To get this right, law schools need to closely engage with those working in practice.
Continuing the experiment, the second core component of CBLE requires competencies and their developmental markers to be sequenced progressively. Within the medical community, sequenced progression has taken the form of a narrative model that tracks the developmental stages from novice to competent graduate. This led to what CBME calls Milestones, which have been built out by the Accreditation Council for Graduate Medical Education (ACGME), the accreditor for residency programs. The ACGME continues to work closely with practicing physicians and professors to create Milestone models for all 24 medical specialties.
To date, the ABA as the accreditor for law schools has shown no interest in providing this type of support for legal education. To fill this void, the Holloran Center has formed working groups that are creating Milestone models on the most common law school learning outcomes beyond technical legal skills. They are available at Holloran Competency Milestone.
The Milestones model
Milestones on a specific competency provide a “shared mental model” of professional development from student to competent practitioner and beyond to mastery. Laura Edgar et al, “Milestones 2.0: A Step Forward,” 10 J. Grad. Med. Educ. 367–69 (2018). The power of this approach is that it defines a logical learning trajectory of professional development and makes transparent significant points in student development. The result is less uncertainty and more efficient communication throughout the learning process.
Indeed, once built and adopted, Milestones can be used for formative and summative assessment for students and overall program assessment. If a faculty and staff adopt a Milestone model for a particular competency, they also are building consensus on what competent performance looks like, which in turn fosters better inter-rater reliability. Finally, Milestones describe what a trajectory should look like so that learners can track their own progress toward a particular competency and programs can recognize which students are in need of extra help.
Figure 2 depicts how Milestones work within the well-known Dreyfus model of development from novice to expert.

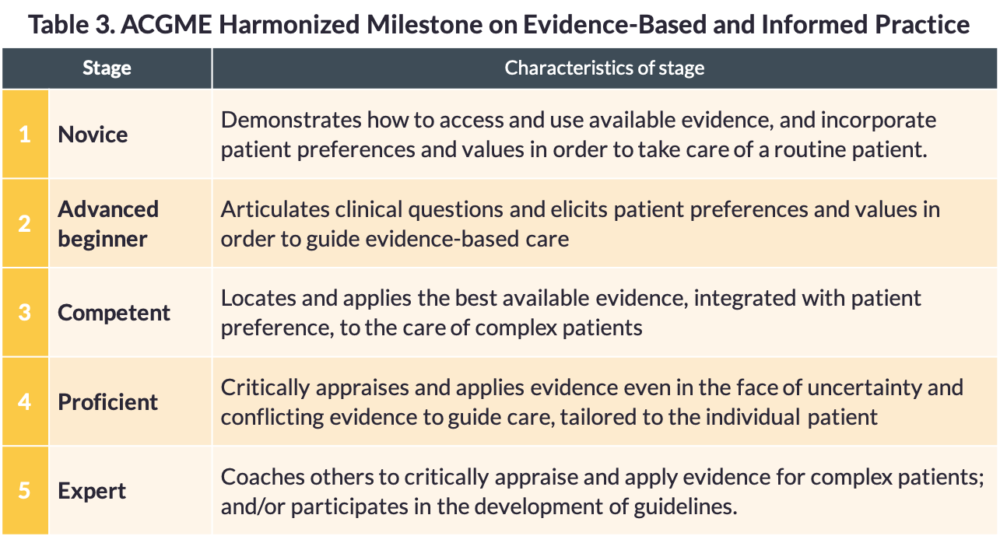
What does this look like in the field? Table 3 presents an ACGME Milestone on patient-centered problem-solving.
Inherent in the Dreyfus and Milestone models is that learners take ownership of their own continuous professional development, particularly at the latter stages of each competency. According to the Guidebook distributed to fellows and residents by ACGME, learners in a competency-based education system “must be active agents co-guiding both the curricular experiences and assessment activities.” Eric Holmboe, MD, et al., The Milestones Guidebook (ACGME 2016) at 15.
What does it mean for a student to be an active agent in her own learning and assessment? “Learners must learn to be self-directed in seeking assessment and feedback.” Holmboe & Englander, supra, at 350. Learners should ideally:
- Be both introduced to the overall competency-based education curriculum at the beginning and engaged in dialogue about the overall program on an ongoing basis;
- Actively seek out assessment and feedback on an ongoing basis;
- Perform regular self-evaluations together with feedback from external sources;
- Direct and perform some of their own assessments such as seeking out direct observation of the learner by an experienced professional and creating portfolios of evidence regarding specific competencies; and
- Develop personal learning plans that students revisit and revise at least twice a year.
Preparing students to enter practice
Medical education has also emphasized the importance of providing coaching and guided reflection at significant transition points for students. This approach is grounded in the belief that new entrants to a profession should be growing, step by step, from being an outsider with a stance of an observer to an insider who has absorbed valuable tacit knowledge. See William Sullivan, “Foreword,” in Teaching Medical Professionalism at ix, xii (Richard Creuss et al. eds. 2d ed. 2016)
Medical professors Lockyer, de Groot and Silver observe:
Generally, transitions are critically intense learning periods associated with a limited time in which a major change occurs and that change results in a transformation. During transitions, people re-form their way-of-being and their identity in fundamental ways. Thus, transitions represent a process, which involves a fundamental reexamination of one’s self, even if the processing occurs at a largely unconscious level. In transition periods, people enter into new groups or “communities of practice.” This involves adopting shared, tacit understandings, developing competence in the skilled pursuit of the practice, and assuming a common outlook on the nature of the work and its context.
Jocelyn Lockyer, et al., “Professional identity formation: the practicing physician, and continuing professional development,” in Teaching Medical Professionalism, supra at 186-88. Medical educators note that these transitions are often characterized by anxiety, stress, and risk for the developing professional. As a long-time legal educator, I believe the same dynamics apply to law students.
So, how do students themselves assess the important transitions in their journey from novice to competent learner/beginning practicing lawyer?
To start answering this question, I developed a Qualtrics survey for law students in September of the 2L year asking them to reflect on the transitions of the 1L year and the summer between the 1L and the 2L years. The survey focused on transitions regarding ownership over continuous professional development. At the University of St. Thomas School of Law, all 2Ls take Professional Responsibility in the 2L year; so, 62 of the 62 2L students in my Professional Responsibility class filled out the survey.
The key survey question read: “In the context of the self-directed learning stage development model, what is the impact of each experience in this survey on your transition from thinking and acting like a student to thinking and acting like a junior lawyer?” The respondent could choose among the following: no impact, some impact, moderate impact, substantial impact, great impact. There was also a question where the respondent could add additional experiences that were significant with respect to this question, but none of the added experiences had more than one respondent.
Figure 3 indicates the experiences that had the greatest impact.
![]()
Summer employment experience (paid or unpaid) after the 1L year is a singularly important professionally authentic transition. Note that summer employment is currently completely outside of the formal curriculum, but the law school should provide some coaching and guided reflection and guided self-assessment for each student about the summer employment transition experience.
Law schools should also provide some coaching and guided reflection at other significant transitions where student have authentic professional experiences (real-life or mimicking real-life) in the 2L and 3L years like: (1) all work experiences, paid or unpaid, especially the summer work experiences; (2) clinic and externship experiences; and (3) simulation experiences.
Conclusion
Over 20 years ago, medical education embarked upon a mission to upgrade the quality of its education, primarily because a large number of patients were being put in harm’s way by young doctors who were graduating underskilled from medical school. What are the odds that legal education does not suffer from similar deficiencies?
Fortunately, our peers in medical education have provided us with a valuable roadmap for how to navigate our journey toward competency-based professional education.